Medical Dermatology
Medical Dermatology
(Chronic & Inflammatory Skin Diseases)
 Skin Cancer & Pre-Cancer Care
Skin Cancer & Pre-Cancer Care
Medical Dermatology
(Chronic & Inflammatory Skin Diseases)
- Acne & Acne Scarring
- Rosacea
- Psoriasis (includes Excimer laser, Narrow band UVB phototherapy)
- Eczema (Atopic Dermatitis)
- Seborrheic Dermatitis
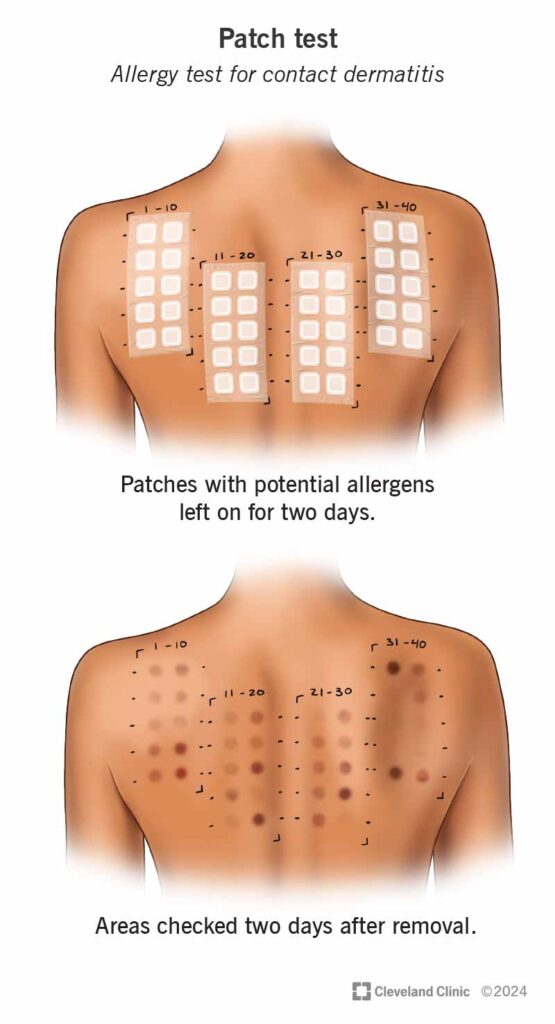
Contact Dermatitis
- Hives (Urticaria)
- Vitiligo (includes Excimer laser, Narrow band UVB phototherapy)
- Hair Loss (Alopecia)
- Pruritus (Chronic Itching)
- Autoimmune Skin Disorders
- Warts, Molluscum, Fungal
- Sarcoidosis (Skin Involvement)
- Hyperhidrosis (Excessive Sweating)
- Lichen planus
- Blistering Skin Disorders
- Bacterial Skin Infections
- Keloids (Overgrown scar)
- Paraneoplastic Dermatoses (a clue to an internal cancer)
- Skin Issues Related to STDs (STIs)
- Scabies
 Pigment & Lesion Disorders
Pigment & Lesion Disorders
 Non-Cancer Growth
Non-Cancer Growth
 Surgical Dermatology (Non-Cancer Procedures)
Surgical Dermatology (Non-Cancer Procedures)
 Cosmetic Dermatology
Cosmetic Dermatology