 Medical Dermatology
Medical Dermatology
(Chronic & Inflammatory Skin Diseases)
 Skin Cancer & Pre-Cancer Care
Skin Cancer & Pre-Cancer Care
Medical Dermatology
(Chronic & Inflammatory Skin Diseases)
- Acne & Acne Scarring
- Rosacea
- Psoriasis (includes Excimer laser, Narrow band UVB phototherapy)
- Eczema (Atopic Dermatitis)
- Seborrheic Dermatitis
- Contact Dermatitis
- Hives (Urticaria)
- Vitiligo (includes Excimer laser, Narrow band UVB phototherapy)
- Hair Loss (Alopecia)
- Pruritus (Chronic Itching)
Autoimmune Skin Disorders
- Warts, Molluscum, Fungal
- Sarcoidosis (Skin Involvement)
- Hyperhidrosis (Excessive Sweating)
- Lichen planus
- Blistering Skin Disorders
- Bacterial Skin Infections
- Keloids (Overgrown scar)
- Paraneoplastic Dermatoses (a clue to an internal cancer)
- Skin Issues Related to STDs (STIs)
- Scabies
 Pigment & Lesion Disorders
Pigment & Lesion Disorders
 Non-Cancer Growth
Non-Cancer Growth
 Surgical Dermatology (Non-Cancer Procedures)
Surgical Dermatology (Non-Cancer Procedures)
 Cosmetic Dermatology
Cosmetic Dermatology
• Autoimmune Skin Disorders
(When the immune system mistakenly targets the skin)
What Are Autoimmune Skin Disorders?
Autoimmune skin disorders are conditions where your immune system becomes overactive and mistakenly attacks parts of your body—such as the skin, hair follicles, blood vessels, or connective tissue. This can lead to rashes, blisters, sores, color changes, or scarring.
These conditions are not contagious, and many can be well-managed with the right diagnosis and treatment plan.
Common Autoimmune Skin Conditions We Evaluate
Autoimmune skin disorders can look very different. Examples include:
1) Inflammatory rashes
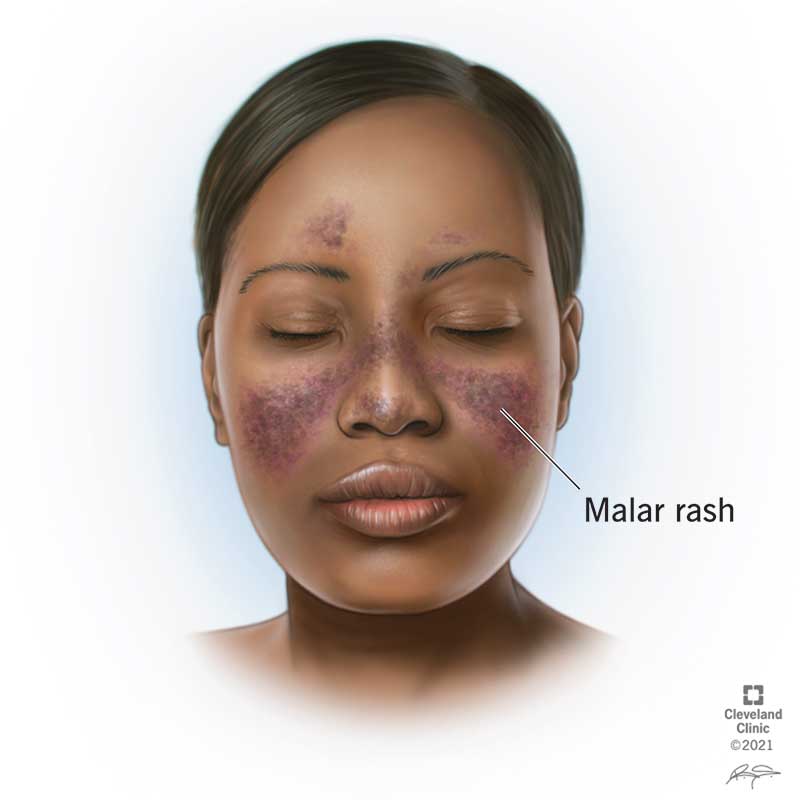
Cutaneous lupus (often sun-sensitive rashes)
Dermatomyositis (rash with possible muscle weakness)

2) Blistering autoimmune conditions
Bullous pemphigoid (tense blisters, often very itchy)
Pemphigus (more fragile blisters/erosions)
3) Blood vessel inflammation
Cutaneous vasculitis (often purple spots on legs, sometimes tender)
4) Pigment and hair-related autoimmune conditions
Vitiligo (white patches)
Alopecia areata (patchy hair loss)
5) Connective tissue autoimmune conditions
Scleroderma/morphea (firm, thickened patches)
Important: Many non-autoimmune conditions can mimic autoimmune rashes—so proper evaluation matters.
Typical Symptoms
You may notice:
A rash that persists, spreads, or keeps returning
Sun sensitivity (rash worsens after sun exposure)
Blisters, open sores, crusting, or painful erosions
Purple spots or bruising-like marks, especially on legs
Scalp tenderness or patchy hair loss
Mouth sores or lip involvement
Burning, stinging, or intense itching
Nail changes
How We Diagnose Autoimmune Skin Disorders
Diagnosis usually involves a combination of:
1) Detailed history
We ask about:
When the rash started and how it behaves
Medications and recent changes
Sun exposure patterns
Joint pain, fatigue, fevers, muscle weakness, mouth sores
Family history of autoimmune disease
2) Full skin exam
We look for pattern clues (location, shape, color, scale, blisters).
3) Skin biopsy (often key)
A small sample of skin is taken to examine under the microscope.
Sometimes a special test called direct immunofluorescence (DIF) is needed (especially for blistering disorders).
This requires a specific biopsy technique and location—your dermatologist will guide this.
4) Blood tests (when appropriate)
Used to look for inflammation markers, autoimmune antibodies, or to help rule in/out systemic involvement.
5) Coordination with other specialists
If needed, we coordinate care with rheumatology, pulmonology, neurology, or ophthalmology depending on symptoms.
Treatment Options
Treatment depends on the diagnosis, severity, and whether other organs are involved.
1) Skin-directed treatments
Gentle skin care + anti-inflammatory prescription creams/ointments
Sun protection plans (critical for many autoimmune rashes)
Wound care for sores or erosions
2) Systemic treatments (when needed)
For more significant disease, treatments may include oral or injectable medications that calm the immune system. Your dermatologist will discuss:
Benefits and risks
Monitoring needs (labs, infection prevention, vaccines when appropriate)
Pregnancy considerations (if relevant)

Pre-Op Instructions (Before Your Autoimmune Rash Visit / Biopsy)
(Not surgery—these are “before your appointment” tips.)
Before your visit
Take photos of the rash when it’s flaring (many rashes change day-to-day).
Bring a list of:
All medications and supplements (including OTC and “natural” products)
New products that touch your skin (soaps, creams, cosmetics)
Write down any “whole-body” symptoms:
Fatigue, fevers, joint pain, muscle weakness
Mouth sores, eye irritation
Shortness of breath or chest symptoms
If a biopsy may be done
Tell us if you take blood thinners or bruise easily.
⚠️ Do not stop prescribed blood thinners unless your prescribing clinician instructs you.
Tell us about allergies to adhesives, antiseptics, or numbing medicine.
Post-Op Instructions (After Biopsy / Starting Treatment)
If you had a biopsy
Keep the bandage on and dry for 24 hours (unless instructed otherwise).
After 24 hours, daily:
Gently clean with mild soap and water
Pat dry
Apply a thin layer of ointment if instructed
- Cover with a clean bandage
Avoid soaking (pools/hot tubs/baths) until healed.
Call if you have increasing redness, warmth, swelling, pus, fever, or bleeding that won’t stop with pressure.
When to Seek Urgent Care
Seek urgent or emergency care if you have:
Trouble breathing, chest pain, severe weakness, or confusion
Rapidly spreading blisters, skin pain, or widespread skin peeling
Swelling of lips/tongue/throat or difficulty swallowing
High fever with rapidly worsening rash
Call our office promptly if:
New blisters, sores in the mouth/eyes, or rapidly worsening symptoms
Signs of infection in open skin (increasing pain, pus, fever)
Frequently Asked Questions
Are autoimmune skin disorders contagious?
No. You cannot catch an autoimmune skin disorder from someone else.
Does an autoimmune rash mean I have a systemic autoimmune disease?
Not always. Some conditions are limited to the skin, while others can involve internal organs. Your dermatologist will evaluate symptoms and testing to clarify this.
Why is a biopsy important?
Many rashes look similar on the surface. A biopsy can provide the most accurate diagnosis and guide the safest, most effective treatment.
What is DIF (direct immunofluorescence)?
DIF is a special biopsy test that looks for immune proteins in the skin—especially helpful for autoimmune blistering disorders.
Will I need blood tests?
Sometimes. Blood tests can help confirm certain diagnoses, assess inflammation, and screen for systemic involvement.
Can stress trigger flares?
Stress may worsen inflammation and trigger flares in some autoimmune conditions. Managing stress can be a helpful part of an overall plan.
Will sun exposure make it worse?
For several autoimmune disorders (especially some forms of lupus), sun can trigger or worsen rashes. We’ll give you a sun protection plan tailored to your condition.
Are treatments safe long-term?
Many treatments can be used safely with proper monitoring. If immune-suppressing medication is needed, we’ll discuss side effects, infection precautions, and lab monitoring.
How soon will I see improvement?
It depends on the diagnosis and severity. Some patients improve in 1–2 weeks, while others require several weeks to months and a maintenance plan.