Skin Cancer & Pre-Cancer Care
Skin Cancer & Pre-Cancer Care
B. Skin Cancer Types
Skin Cancer & Pre-Cancer Care
A. Skin Cancer Diagnosis
B. Skin Cancer Types
- Basal Cell Carcinoma (BCC)
- Squamous Cell Carcinoma (SCC)
- Melanoma
- Merkel Cell Carcinoma
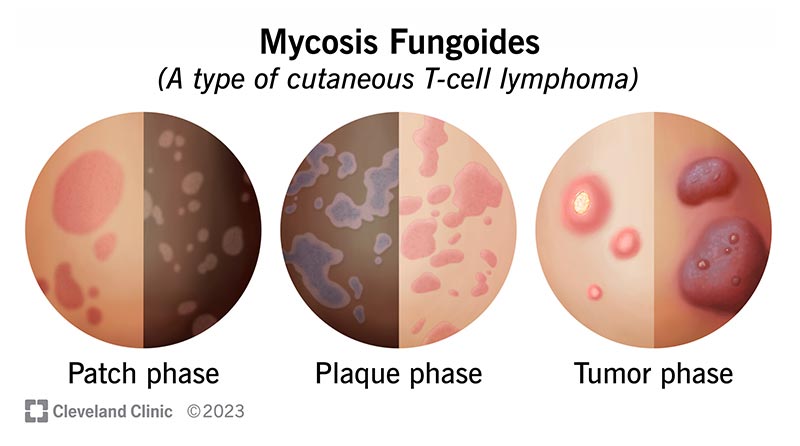
Cutaneous T-Cell Lymphoma (CTCL)
- Primary Cutaneous B-Cell Lymphoma (PCBCL)
- Metastatic Cancers
- Sarcoma
C. Skin Cancer Treatment
- Mohs Micrographic Surgery
- Surgical Excision
- Electrodessication & Curettage(ED&C)
- Radiation Referral Coordination
D. Pre-Cancerous Lesions
- Actinic Keratosis (AK)
- Atypical(Dysplastic) Nevi
- Field Cancerization Treatment
- Photodynamic Therapy (PDT)
 Medical Dermatology
Medical Dermatology
(Chronic & Inflammatory Skin Diseases)
 Pigment & Lesion Disorders
Pigment & Lesion Disorders
 Non-Cancer Growth
Non-Cancer Growth
 Surgical Dermatology (Non-Cancer Procedures)
Surgical Dermatology (Non-Cancer Procedures)
 Cosmetic Dermatology
Cosmetic Dermatology