 Skin Cancer & Pre-Cancer Care
Skin Cancer & Pre-Cancer Care
B. Skin Cancer Types
Skin Cancer & Pre-Cancer Care
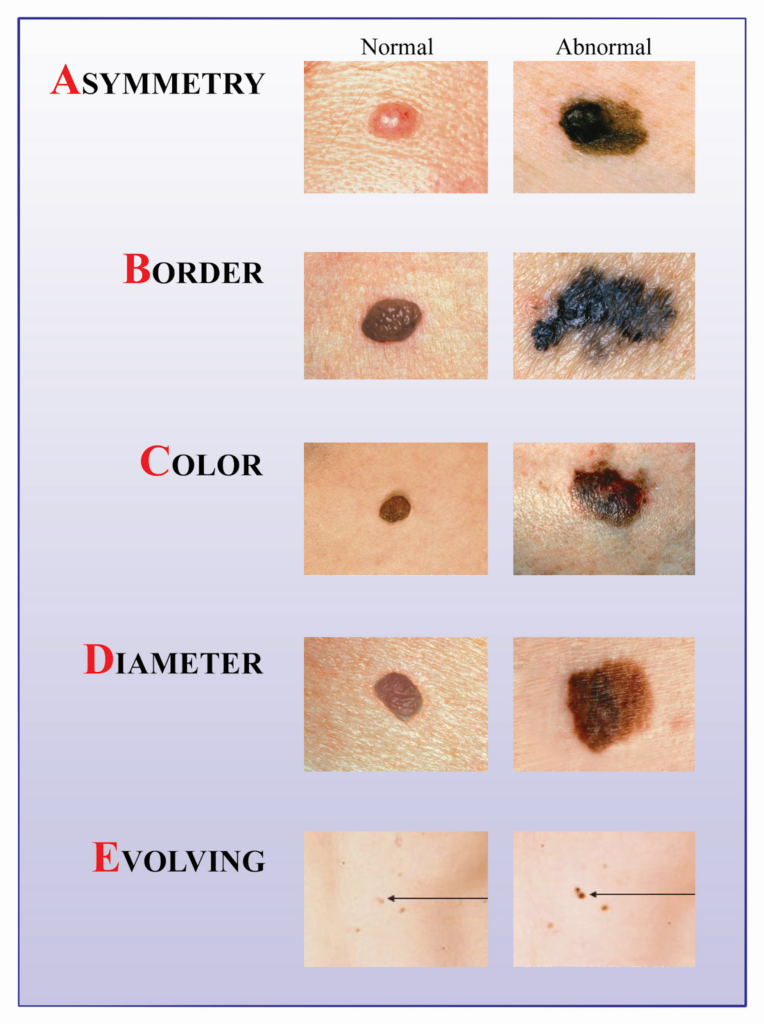
A. Skin Cancer Diagnosis
B. Skin Cancer Types
- Basal Cell Carcinoma (BCC)
- Squamous Cell Carcinoma (SCC)
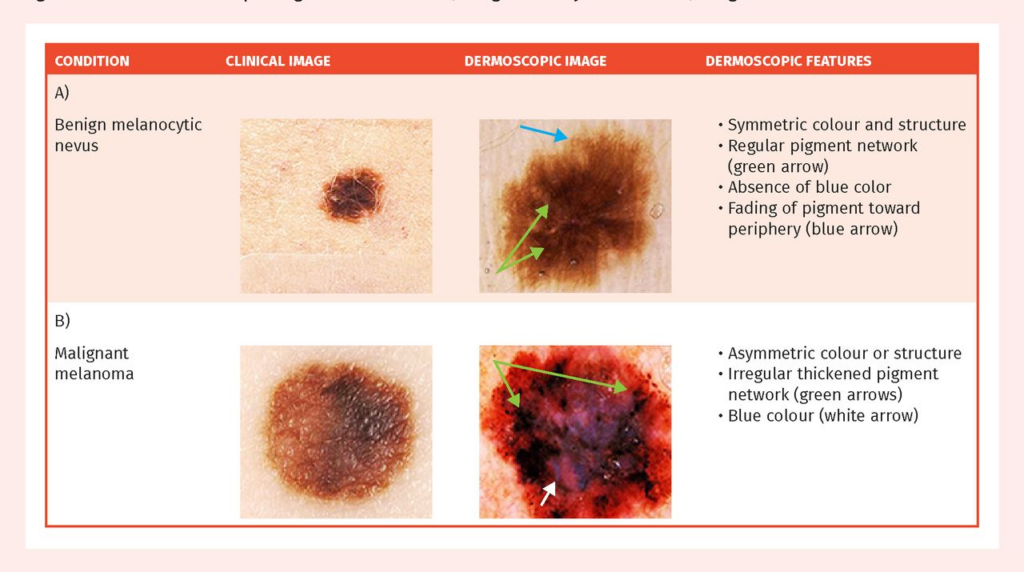
Melanoma
- Merkel Cell Carcinoma
- Cutaneous T-Cell Lymphoma (CTCL)
- Primary Cutaneous B-Cell Lymphoma (PCBCL)
- Metastatic Cancers
- Sarcoma
C. Skin Cancer Treatment
- Mohs Micrographic Surgery
- Surgical Excision
- Electrodessication & Curettage(ED&C)
- Radiation Referral Coordination
D. Pre-Cancerous Lesions
- Actinic Keratosis (AK)
- Atypical(Dysplastic) Nevi
- Field Cancerization Treatment
- Photodynamic Therapy (PDT)
 Medical Dermatology
Medical Dermatology
(Chronic & Inflammatory Skin Diseases)
 Pigment & Lesion Disorders
Pigment & Lesion Disorders
 Non-Cancer Growth
Non-Cancer Growth
 Surgical Dermatology (Non-Cancer Procedures)
Surgical Dermatology (Non-Cancer Procedures)
 Cosmetic Dermatology
Cosmetic Dermatology
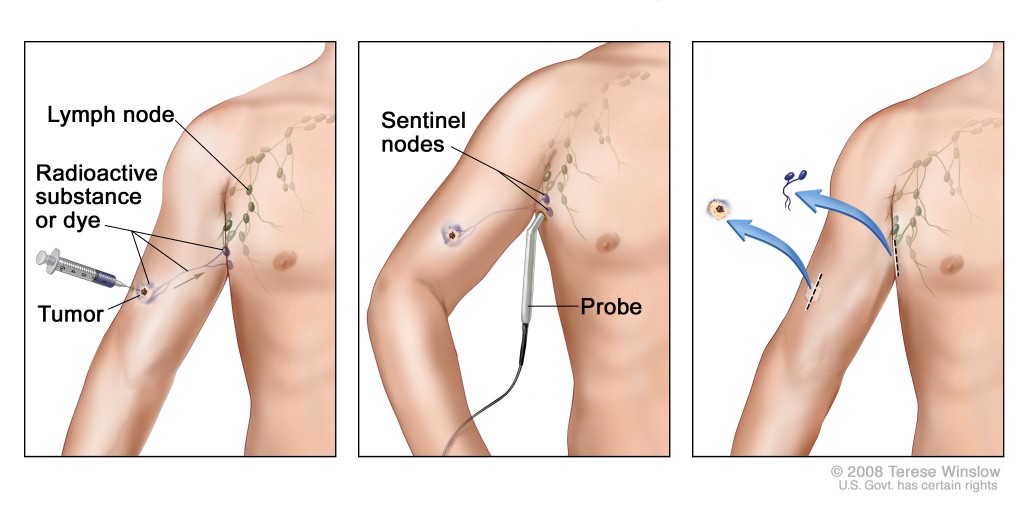
 Important to Know About Where SLNB Is Done
Important to Know About Where SLNB Is Done
- SLNB is NOT performed in our dermatology office
- It is done by an oncologic general surgeon
- The procedure is performed in an operating room (OR) setting
It involves lymphatic mapping using specialized imaging (often nuclear medicine guidance)
We coordinate your care and refer you to the appropriate surgical team when SLNB is recommended.
If melanoma is more advanced, additional treatments may include systemic therapies (such as immunotherapy or targeted therapy) coordinated with oncology.