 Skin Cancer & Pre-Cancer Care
Skin Cancer & Pre-Cancer Care
D. Pre-Cancerous Lesions
Skin Cancer & Pre-Cancer Care
A. Skin Cancer Diagnosis
B. Skin Cancer Types
- Basal Cell Carcinoma (BCC)
- Squamous Cell Carcinoma (SCC)
- Melanoma
- Merkel Cell Carcinoma
- Cutaneous T-Cell Lymphoma (CTCL)
- Primary Cutaneous B-Cell Lymphoma (PCBCL)
- Metastatic Cancers
- Sarcoma
C. Skin Cancer Treatment
- Mohs Micrographic Surgery
- Surgical Excision
- Electrodessication & Curettage(ED&C)
- Radiation Referral Coordination
D. Pre-Cancerous Lesions
- Actinic Keratosis (AK)
Atypical(Dysplastic) Nevi
- Field Cancerization Treatment
- Photodynamic Therapy (PDT)
 Medical Dermatology
Medical Dermatology
(Chronic & Inflammatory Skin Diseases)
 Pigment & Lesion Disorders
Pigment & Lesion Disorders
 Non-Cancer Growth
Non-Cancer Growth
 Surgical Dermatology (Non-Cancer Procedures)
Surgical Dermatology (Non-Cancer Procedures)
 Cosmetic Dermatology
Cosmetic Dermatology
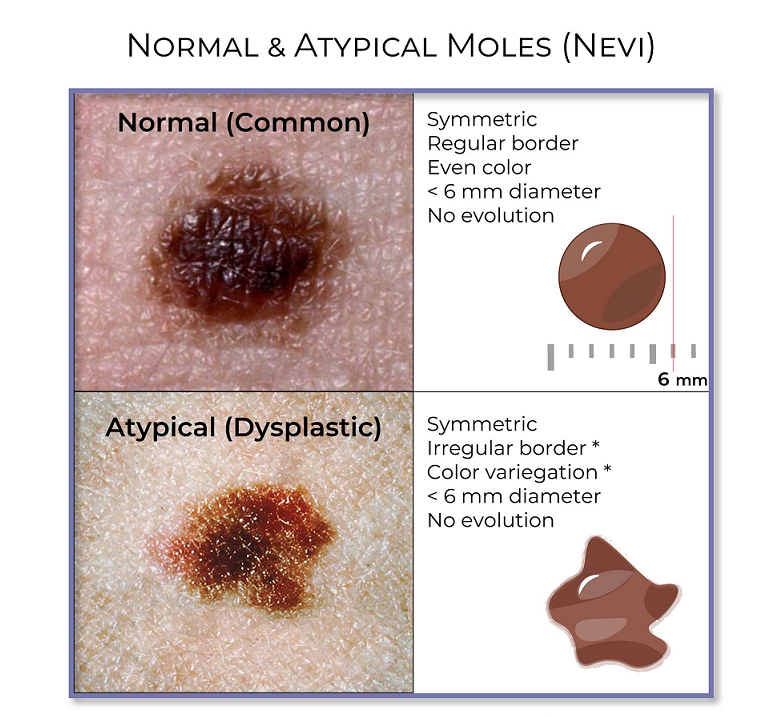
• Atypical (Dysplastic) Nevi - (Atypical Moles)
What Are Atypical (Dysplastic) Nevi?
Atypical nevi (also called dysplastic nevi) are moles that look different from common benign moles. They are not skin cancer, but they can sometimes resemble melanoma and may be a marker that a person has a higher risk of melanoma, especially if they have many atypical moles or a family history of melanoma.
Atypical moles often have one or more of these features:
Asymmetry (one half doesn’t match the other)
Irregular borders
Multiple colors (tan, brown, pink, darker brown)
Larger size than a typical mole
Change over time

Why Atypical Moles Matter
Atypical moles are important because:
Some can be difficult to distinguish from melanoma by appearance alone
People with multiple atypical moles may have a higher lifetime melanoma risk
Monitoring changes over time helps detect melanoma early, when it’s most treatable
How Atypical Moles Are Evaluated
Your dermatologist may recommend one or more of the following:
a) Full-Body Skin Exam
A head-to-toe skin check to evaluate existing moles and look for new or changing lesions.
b) Dermoscopy
A handheld magnifying device that lets your dermatologist see pigment patterns not visible to the naked eye.
c) Digital Monitoring / Mole Mapping (when appropriate)
Photos and/or dermoscopic images may be stored to compare changes over time.
d) Skin Biopsy (if a mole is concerning)
A small sample is removed and examined under the microscope by a dermatopathologist to confirm the diagnosis and determine next steps.
Do Atypical Moles Need to Be Removed?
Not always. Management depends on:
How the mole looks clinically
Whether it is changing
Your personal and family history
The biopsy result (if biopsied), including the degree of atypia and whether margins are clear
Some atypical moles are safely monitored, while others are removed if they are concerning or show significant atypia.
Pre-Op Instructions
(For evaluation, photography/mole mapping, and possible biopsy/excision)
Before Your Appointment
Make note of any spots that are new, changing, bleeding, itching, or different
Bring any history of:
Prior biopsies or skin cancers
Family history of melanoma
Immunosuppression or organ transplant (if applicable)
Day of Your Visit
Wear comfortable clothing
Avoid heavy makeup or body oils if possible (helps visualization)
Remove nail polish if you can (nails can be part of skin screening)
Tie up long hair or bring a clip for scalp evaluation
If you are scheduled for mole mapping: avoid self-tanner and come with clean skin
If a Biopsy Is Planned or Possible
Please tell us if you:
Take blood thinners (aspirin, warfarin, clopidogrel, apixaban, rivaroxaban, etc.)
Have a bleeding disorder or bruise easily
Have allergies to lidocaine, adhesives, or antiseptics
⚠️ Do not stop prescribed blood thinners unless your prescribing clinician instructs you.
Post-Op Instructions
(If a biopsy or excision was performed)
Wound Care
Keep the bandage on and dry for the first 24 hours (unless instructed otherwise)
After 24 hours, daily:
Wash hands
Gently clean with mild soap and water
Pat dry
Apply a thin layer of ointment if instructed
Cover with a clean bandage
Continue until healed or until stitches are removed.
Activity
Avoid heavy exercise, stretching, or friction on the area as instructed—especially if stitches were placed
Avoid soaking (baths, pools, hot tubs) until cleared
Bleeding
If bleeding occurs:
Apply firm pressure for 15 minutes without checking
Repeat once if needed
If still bleeding after 30 minutes, contact the office
Call the Office If You Notice
Increasing redness, warmth, swelling, pus, or fever
- Worsening pain after the first day
The wound opens or stitches come loose
Results & Next Steps
Biopsy results are often available within several business days (timing varies). We will contact you with:
The diagnosis
Whether additional treatment is needed
A personalized follow-up plan (monitoring vs removal)
Frequently Asked Questions
Are atypical (dysplastic) moles cancer?
No. Atypical moles are benign, but they can look similar to melanoma and may indicate a higher melanoma risk in some patients.
Does having atypical moles mean I will get melanoma?
Not necessarily. Many people with atypical moles never develop melanoma, but the risk can be higher—especially with many atypical moles and/or a family history of melanoma. Regular skin exams help with early detection.
How do I know if one of my moles is concerning?
Use the ABCDE warning signs:
Asymmetry
Border irregularity
Color variation
Diameter growth
Evolving (changing)
Also watch for the “ugly duckling” mole—one that looks noticeably different from your other moles.
Do atypical moles have to be removed?
No. Some are monitored safely. Removal is recommended when a mole appears suspicious, changes over time, or shows significant atypia on biopsy.
What is dermoscopy and why is it used?
Dermoscopy is a magnified exam with specialized light that helps dermatologists evaluate pigment patterns more accurately and decide whether a mole should be monitored or biopsied.
What is mole mapping, and do I need it?
Mole mapping uses total-body photography and/or digital dermoscopy images to track moles over time. It’s most helpful for patients with many moles, atypical moles, or higher melanoma risk.
If a biopsy shows “mild, moderate, or severe atypia,” what does that mean?
It describes how unusual the mole cells look under the microscope. Management depends on the level of atypia, whether the entire lesion was removed, and clinical context. Your dermatologist will explain your specific result and recommended next step.
Will a biopsy or removal leave a scar?
Any procedure can leave a small scar. Good wound care and sun protection during healing help scars fade more evenly over time.
How often should I have skin checks if I have atypical moles?
That depends on your risk factors (number of moles, family history, prior skin cancer, etc.). Your dermatologist will recommend a schedule—often ranging from periodic to more frequent exams for higher-risk patients.