
• Sentinel Lymph Node Biopsy Coordination
(Referral coordination for melanoma staging when lymph node evaluation is needed)
What Is Sentinel Lymph Node Biopsy?
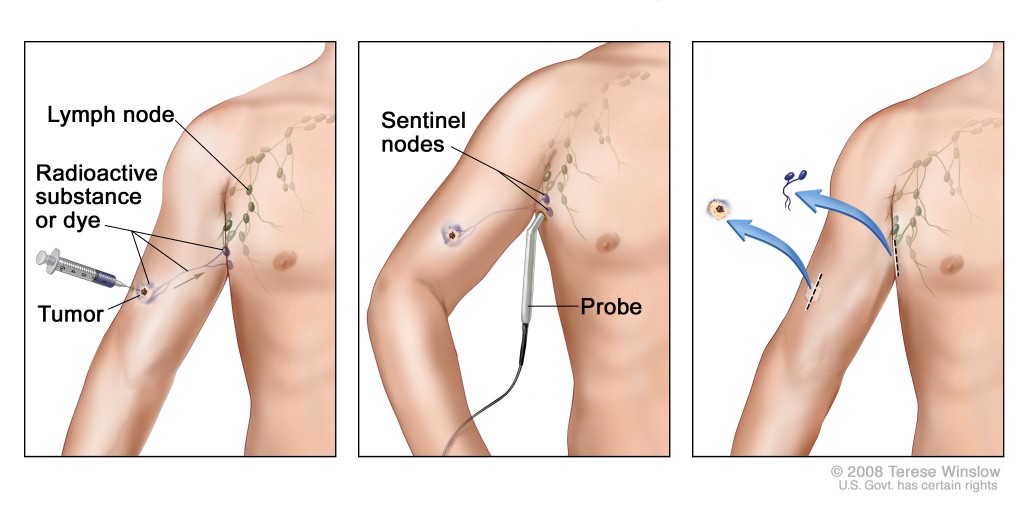
A sentinel lymph node biopsy (SLNB) is a specialized procedure used in some patients with melanoma to determine whether cancer cells have spread to the nearest draining lymph node. The sentinel node is the first lymph node that receives drainage from the melanoma site, so testing it helps determine the melanoma stage and guide next steps in care.
Our Role: Coordination, Not In-Office SLNB
Our dermatology office does not perform sentinel lymph node biopsy in the office. When SLNB is recommended, we coordinate referral to an oncologic general surgeon or melanoma surgical specialist because the procedure is performed in an operating room setting, often with lymphatic mapping support. Lymphatic mapping may involve injection of a tracer near the melanoma site to identify the sentinel node location before surgery
When Is SLNB Considered?
SLNB is not needed for every melanoma. It may be considered based on melanoma features such as:
- Breslow depth / tumor thickness
- Ulceration
- Mitotic rate or other high-risk pathology findings
- Location and clinical risk factors
Your dermatologist will review your biopsy report and explain whether SLNB discussion is appropriate for your case.
Why SLNB Matters
SLNB helps:
- Determine melanoma stage more accurately
- Identify whether melanoma has reached nearby lymph nodes
- Guide oncology referral, imaging, surveillance, or additional treatment if needed
- Provide important prognostic information
A negative SLNB suggests melanoma has not spread to nearby lymph nodes, while a positive SLNB may indicate stage III melanoma and the need for additional care planning.
What to Expect During Coordination
Our team may help with:
- Reviewing your melanoma pathology report
- Explaining why SLNB is or is not recommended
- Sending records to the surgical specialist
- Coordinating with oncology, surgical oncology, or general surgery
- Continuing long-term skin surveillance after treatment
Pre-Op Instructions
General guidance before your surgical consultation or SLNB. Follow the surgeon’s exact instructions if they differ.
- Bring your melanoma pathology report, medication list, allergy list, and insurance information.
- Tell the surgical team if you take blood thinners, aspirin, NSAIDs, supplements, or have a bleeding disorder.
- Do not stop prescription medications unless instructed by your prescribing clinician or surgical team.
- Follow fasting instructions if the procedure will be done under anesthesia.
- Arrange transportation if sedation or anesthesia is used.
- Ask where lymphatic mapping will be performed and whether it occurs before or on the same day as surgery.
Post-Op Instructions
Follow your surgeon’s instructions first.
After SLNB, patients may have:
- Mild soreness near the incision
- Bruising or swelling
- Temporary tightness or tenderness
- A small scar near the lymph node biopsy site
General aftercare:
- Keep the incision clean and dry as directed.
- Avoid strenuous activity until cleared by the surgeon.
- Watch for increasing redness, warmth, pus, fever, worsening pain, or swelling.
- Attend all follow-up visits to review pathology results and next steps.
Frequently Asked Questions
Is SLNB done in your dermatology office?
No. SLNB is performed by an oncologic/general surgeon or melanoma surgical specialist in an operating room setting.
Does needing SLNB mean my melanoma has spread?
No. SLNB is a staging test. Many patients have a negative result.
What is lymphatic mapping?
Lymphatic mapping helps identify which lymph node drains the melanoma area first. A tracer is injected near the tumor site and imaging helps map the drainage pathway.
What happens if the sentinel node is negative?
A negative result is reassuring and suggests melanoma has not spread to nearby lymph nodes. Follow-up skin exams and surveillance are still important.
What happens if the sentinel node is positive?
A positive result means melanoma cells were found in the node. Your care team may recommend oncology referral, imaging, additional treatment discussion, and closer surveillance.
Will I still see my dermatologist after SLNB?
Yes. Dermatology follow-up remains essential for full-body skin exams, melanoma surveillance, and monitoring for new or changing lesions.
Is SLNB the same as removing all lymph nodes?
No. SLNB usually removes only the first draining lymph node or small group of nodes for testing.